


1Clalit Health Services, Yavne, 2Siaal Research Center for Family Medicine and Primary Care, Division of Community Health, Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, 3Department of Dermatology, Rambam Health Care Campus, Haifa, Israel, 4Department of Non-communicable Disease Epidemiology, Faculty of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, UK, 5Department of Family Medicine, Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, Clalit Health Services, 6Department of Family Medicine, Rabin Medical Center, Petah Tikva, Israel, 7Pediatric unit, Department of Dermatology and Venereology, Soroka Medical Center; Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, 8Department of Quality Measurements and Research, Chief Physician’s Office, Clalit Health Services, Tel-Aviv, 9Department of Medicine ‘B’, Sheba Medical Center, Tel-Hashomer, Ramat-Gan, Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, and 10Department of Dermatology, HaEmec MC, Afula, Israel
Understanding of the epidemiology and healthcare service utilization related to atopic dermatitis is necessary to inform the use of new treatments. This cross-sectional study was based on a group of patients with atopic dermatitis and a matched control group comprised of age- and sex- matched enrolees without atopic dermatitis from a large medical database. Healthcare service utilization usage data were extracted and compared between groups. The study included 116,816 patients with atopic dermatitis and 116,812 controls. Atopic dermatitis was associated with an increased burden of healthcare utilization across the entire spectrum of healthcare services compared with controls. For patients severely affected by atopic dermatitis, the increased burden correlated with disease severity: a high-er frequency of emergency room visits (odd ratio (OR) 1.7; 95% confidence interval (CI) 1.6–1.9), dermatology wards hospitalizations (OR 315; 95% CI 0–7,342), and overall hospitalizations (OR 3.6; 95% CI 3.3–3.9). In conclusion, this study demonstrates an increased burden of healthcare utilization in atopic dermatitis.
Key words: atopic dermatitis; healthcare service utilization; epidemiology.
Accepted Jan 16, 2019; E-published Jan 22, 2018
Acta Derm Venereol 2019; 99: XX–XX.
Corr: Guy Shalom, Clalit Health Services, 2nd Snapir St., 8155211 Yavne, Israel. E-mail: guyshal@post.bgu.ac.il
Treatment arsenal for atopic dermatitis has expanded dramaticly during last years. To allow the incorporation of the newly introduced, expensive treatments the epidemiology and healthcare service utilization of patients with atopic dermatitis must be defined in a timely manner. We report an increased burden of healthcare utilization across the entire spectrum of healthcare services in a large group of 116,816 patients with atopic dermatitis compared with controls without atopic dermatitis. Increased emergency room visits, hospitalizations in dermatology wards, and overall hospitalizations were found. A dose-response manner according to disease severity was observed.
Atopic dermatitis (AD) is a common chronic non-contagious relapsing inflammatory skin disorder. The current prevalence of AD in most high-income and some low-income countries is approximately 10–30% in children and 2–10% in adults (1, 2), yet data regarding healthcare service utilization and drug use in patients with AD are lacking. Until recently, the treatment choices for AD were limited, especially for severe AD. Treatments include long-term emollients and topical steroids as first-line therapy, followed by topical calcineurin inhibitors. Systemic treatments for AD may include antihistamines, but consist mainly of steroids, methotrexate, ciclosporin, azathioprine, mycophenolate mofetil, or phototherapy. All of these have proven effective and can be successful in moderate-to-severe disease (3–6).
Insights regarding the pathogenesis of AD during recent years, have led to the introduction of breakthrough treatments, leading to considerable changes in treatment modalities for AD. Defining the epidemiology, healthcare service utilization, and drug use of patients with AD is necessary to inform the use of these newly introduced treatments. This study investigated the demographic and epidemiological characteristics, healthcare service utilization, and drug usage of a large group of patients with AD in Israel, selected from the medical database at Clalit Health Services (CHS).
CHS is the largest health maintenance organization (HMO) in Israel and one of the largest HMO’s globally, serving a population of over 4,400,000 patients. Dermatology consultations at CHS can take place in 3 different settings; an inpatient setting (hospitalization), an outpatient setting (in a clinic affiliated with a hospital), or in a primary care clinic (with no hospital affiliation, also called a community setting) where the consultation is performed by an independent board-certified specialist. Consultations with a family physician or primary care paediatrician are free of charge. Community-based dermatology consultations are accessible without the need for referral; these involve a small quarterly co-payment (~10 US$). This easy, low-cost accessibility leads to relatively high use of dermatologist consultations in Israel. Consequently, most patients with AD in Israel are evaluated and treated by a dermatologist in the primary care setting; this study therefore focused on the CHS community setting.
At CHS, all prescribed drugs and claimed prescriptions are captured electronically. This does not include over-the-counter (OTC) drugs, such as emollients or those acquired without a physician prescription outside CHS pharmacies. In the latter case, all expenses are out of pocket.
The design was a cross-sectional study of AD patients and an age- and sex-matched comparison group. The AD group consisted of patients with at least one documented diagnosis of AD made by CHS dermatologists in community services, inpatient clinics, and outpatient clinics or during dermatology hospitalizations between 1998 and 2016. Case-patients had at least one of the following diagnoses: AD; atopic eczema; infantile eczema; flexural eczema. A matching control group of participants without AD was selected, frequency-matched by age and sex, from the general population of CHS enrolees. Age-matching was grounded in the exact year of birth (1-year strata). Controls had to be alive and contributing data to CHS on the date of the diagnosis of the matched case.
This study conforms to ethics standards on human experimentation and with the Declaration of Helsinki 1975, revised in 1983. It was approved by the Ethics Review Committee of CHS.
Demographic information extracted from the CHS medical database included age, sex, socioeconomic status (upper, middle, or lower class), smoking status, marital status, ethnicity (Arab or non-Arab), country in which the patient was born (Israel; Europe/North America; Africa/Asia), body mass index (BMI), Charlson’s comorbidity index score upon enrollment (a validated method for classifying comorbid conditions associated with mortality risk) (7), and severity of AD, as defined below according to healthcare utilization criteria.
Healthcare service utilization data included community clinic visits (general practitioner, and paediatric clinic visits) and community consultations (allergy and dermatology clinic visits) during 2013 to 2016. Use of hospital services included emergency room (ER) visits, dermatology ward hospitalizations, and total number of hospitalizations during 2013 to 2016.
Drug use data included pharmacy claims of topical treatments and systemic treatments. Topical treatments included steroids, pimecrolimus and tacrolimus. Systemic treatments included phototherapy (psoralen plus ultraviolet A, ultraviolet B), and Dead Sea climatotherapy); antihistamines; corticosteroids; methotrexate; ciclosporin; azathioprine; and mycophenolate mofetil. Biologic medications were not available in Israel for the treatment of AD during the observation period of this study, and were therefore not included in the analysis. The extraction of drug utilization data was based on the Anatomical Therapeutic Chemical Classification. The codes are detailed in Table SI.
Severity assessment in AD is based on clinical scores, such as the Severity Scoring of Atopic Dermatitis (SCORAD) index. However, these data could not be drawn from the CHS database. Therefore, AD-related healthcare utilization and pharmacy claims were used as a proxy for AD severity. Patients with AD were considered to have moderate-to-severe AD if they had at least one hospitalization due to AD exacerbation or at least one course of systemic AD-related medication (methotrexate, cyclosporine, azathioprine, or mycophenolate mofetil), with more than 2 successive prescriptions over a period of more than 4 weeks or phototherapy treatment specifically prescribed for AD.
To avoid false-positive cases of moderate-to-severe AD, systemic corticosteroids were not included in this assessment. In addition, for the AD-related medications to be truly relevant to AD severity, the assessment included only drugs that were first initiated close to a diagnosis of AD (i.e. in the same month in which an AD diagnosis was made by a dermatologist); cases in which the drugs were claimed before the first AD signal were not considered moderate-to-severe.
To verify the assessment of severity, a manual search was performed in a sample of files of patients with moderate-to-severe AD. Patients were considered true positive when they had at least one of the following: recorded involvement of 10% body surface area or more, more than 14 cumulative days of sick leave per year, or more than 3 quarterly visits to the dermatologist clinic due to AD.
Data were presented for the entire study population and the matched control group, stratified by disease severity for adults aged 18 years or older. Healthcare utilization and drug use were calculated per patient for both cases and controls in each investigated group and compared using univariate and multivariate regression analyses, adjusted for age, sex, obesity, and smoking. Log-transformations were performed on the odds ratios before conducting these analyses in order to account for non-normality. Data were described for the entire study population and for each subgroup.
Continuous variables were compared using t-tests, and dichotomous variables were compared using a Pearson’s χ2 test. Given the large sample size utilized in the current study, and based on the central limit theorem, it was assumed that the sum of the continuous variables tends toward a normal distribution even if the original variables themselves are not normally distributed. Statistical analysis was performed using SPSS version 23 (SPSS Inc., Chicago, IL, USA). A p-value less than 0.05 was considered statistically significant.
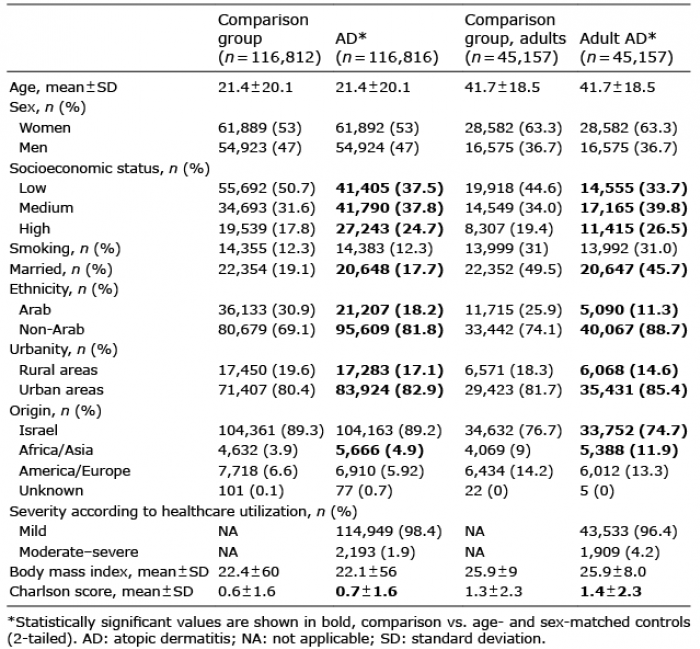
The study included 116,816 Israeli patients with AD and 116,812 age- and sex-matched comparison controls. The results showed that the prevalence of patients with AD amongst the CHS population was 2.7%. Of the individuals with AD, 45,157 were older than 18 years and 1,909 (4.2%) had moderate-to-severe AD. Adult patients with AD were compared with 45,157 adults without AD. Ninety-four files were read, and moderate-to-severe AD was confirmed in 88 patients, a positive predicted value (PPV) of 93.6%. Demographic and clinical characteristics of the study population are shown in Table I. Compared with individuals without AD, patients with AD were more likely to be of high and intermediate socioeconomic status. Patients with AD and adult patients with AD had higher rates of Asian/African origin subjects (4.85% vs. 3.97% and 11.93% vs. 9.01, respectively, p < 0.001), were more likely to live in urban areas (82.9% vs. 80.4% and 85.4% vs. 82.6%, respectively; p < 0.001), and less likely to be married (17.7 vs. 19.1% and 45.7% vs. 48.2%, respectively; p < 0.001). No differences were observed between the groups regarding BMI or Charlson’s comorbidity index scores. The annual healthcare services utilization of patients with AD and of controls during 2013 to 2016 is shown in Table II as mean visits per year per patient. Table III presents the multivariate regression analyses of the relative burden imposed on the healthcare system in terms of healthcare service utilization. The multivariate and univariate analyses gave comparable results. AD patients used the entire spectrum of healthcare services (community services, outpatient services, and hospitalizations), to a greater extent than controls. Drug use according to pharmacy claims data by patients with AD and the general population control group are shown in Table IV. Among patients with AD, topical steroid treatments were the most frequently used topical agent (96% of patients), whereas the most prescribed systemic drugs were antihistamines (85% of patients) and systemic corticosteroids (54% of patients).
Table I. Baseline characteristics of the study population
Table II. Annual healthcare services utilization among patients with atopic dermatitis (AD) and controls 2013 to 2016
Table III. Annual healthcare services utilization among patients with atopic dermatitis and controls 2013–2016, fully adjusted*
Table IV. Annual drug use among controls, study patients with atopic dermatitis (AD) and adult patients with AD 2013 to 2016
This study describes the healthcare burden and drug use associated with AD, based on information obtained from a large community-based healthcare database. The study included 116,816 Israeli patients with AD, representing a prevalence of 2.7% among the CHS enrolled population and 45,157 adults patients with AD, representing a prevalence of 1.5% among the CHS adult population. Univariate and multivariate analyses demonstrated the increased healthcare service, utilization burden, and increased drug use in patients with AD compared with the age- and sex-matched control groups of general population enrolees. The general population comparison group represented the general population of Israel (8). The data obtained quantifies healthcare utilization by patients with AD, and can facilitate incorporation of innovative treatments into the healthcare systems.
In 2010, WHO Global Burden of Disease survey ranked AD most burdensome among common skin diseases, with respect to disability-adjusted life years (9) and years lived with the disease (10). These observations demonstrate the major impact of the disease on healthcare at a population level, albeit the true burden is most probably underestimated because indirect effects, such as psychological effects and comorbidities, were not considered. The economic effects of AD were investigated in a few studies, and the overall medical costs appear to be high (11). A review of 4 studies estimated that the mean direct annual costs could be close to 5 billion USD in 2014. Another conservative estimate of the annual costs of AD in the US by the National Eczema Association is 5.3 billion USD in 2015 (12). Out-of-pocket expenses for OTC products may be up to 10% of household annual income (13). Comorbidities may lever the total annual costs (14, 15) and AD is associated with a wide spectrum of comorbidities (16). The current study quantified the direct burden on healthcare utilization of patients with AD. It was observed that, in comparison with the rest of the population, patients with AD had more than a 5-fold increase in visits to dermatology clinics, more than a 3-fold increase in visits to allergy clinics, and almost 7 times more hospitalizations. Adult patients with severe AD had more than 315 times more hospitalizations in dermatology wards, and 4 times more hospitalizations compared with the general group of AD.
The results of the current study are consistent with those of recent reports on the epidemiology of AD (12, 17–23); however, the current study contributes essential data on community patients. These findings are in line with those of a recent US study that compared adults (≥ 18 years), who self-reported a diagnosis of AD on the 2013 US National Health and Wellness Survey (17). The investigators found that patients with AD put a significantly higher burden on healthcare compared with non-AD controls. The mean ± standard deviation (SD) number of ER visits was 0.5 ± 1.2 for patients with AD; more than twice that for non-AD controls 0.2 ± 0.8 (p < 0.001), and the mean number of hospitalizations was 0.3 ± 1.0 vs. 0.1 ± 0.7 (p = 0.004) for non-AD controls. Patients with moderate-to-severe AD used a greater amount of resources than patients with mild AD; however, in that report none of the differences were statistically significant. Moon et al. assessed the burden of paediatric dermatology consultations in the paediatric emergency department and reported AD to be a leading reason for dermatology consultations in the paediatric emergency department, comprising almost 15% of dermatology consultations in that setting. As a single disease, the most common diagnosis was AD (18). Little is known about inpatient burden and hospitalizations due to AD, yet the small amount of reported data, such as from the National Inpatient Sample, Chicago, Illinois, that reported a substantial inpatient financial burden of AD in the US, are in line with the current report (19).
The validity of AD diagnoses in the present study can be supported by several observations and findings. Abuabara et al. (24) found that at least one out of 5 diagnosis codes plus 2 treatment codes for any skin-directed therapy were likely to accurately identify patients with AD. The authors used codes entered by the physician in general, and not only those entered by dermatologists. The case-patients in the current study had codes entered only by dermatologists, thus providing increased sensitivity. Based on the study of Abuabara et al. (24) we can ascertain the validity of our methods. The general frequency of 2.7% is consistent with the expectation of the prevalence in registry-based studies. In addition, the observed demographic characteristics fit the epidemiological features of AD. Silverwood et al. (25) observed an increased risk of cardiovascular outcomes in severe AD. The investigators used healthcare service utilization and prescribed treatments to evaluate the severity of AD and our definition of severe AD is based on their methodology. The similarity between our methodology and that of Silverwood et al., together with our manual search, strengthen the power of our evaluation of severity. Finally, healthcare services and drug usage profiles of the present group with AD are aligned with the expected profile of the disease. Patients of high and intermediate socioeconomic status were over-represented in the AD group, as expected. These socioeconomic classes are less likely to utilize the healthcare system than those of low socioeconomic status but, in fact, higher utilization was observed in our AD group, further strengthening our conclusions. Taken collectively, the similarities and correlation together with the higher specificity attributable to our case definition, are all suggestive of high validity.
This large registry-based study focussed on primary care and community settings. It reports real-life observations on healthcare utilization by patients with AD, which is its main advantage.
This study also has some limitations; firstly, it has a retrospective design. Secondly, it is based on digitally transmitted data with high specificity; therefore, undiagnosed cases of patients with AD are not included, resulting in an underestimation of the true frequency of AD. This limitation is not unique to this study; it is common among all recent epidemiological registry-based studies. Usage of OTC drugs could not be assessed. The data required to assess disease severity according to the SCORAD index could not be drawn from the CHS database. An attempt to address this limitation was made by evaluating disease severity by proxy, based on healthcare service utilization and prescribed treatments. As in any cross-sectional study, incidence prevalence bias is also a potential limitation. Detection bias is another limitation, as patients with AD tend to interact more intensively with their healthcare provider. Despite these limitations, the study provides important data about the burden of healthcare service utilization and drug use in patients with AD in a general healthcare setting.
Recent advances in the treatment of AD have ushered in a new era of management for this disease. Accumulating evidence on the safety of biologic treatments increases the possibility of better compliance, better clearance, and fewer adverse events. However, these treatments are associated with higher costs. Updated information on health-care services and drug utilization in community-based groups of patients with AD, as presented here, is needed to inform the incorporation of these treatments and other therapies into the healthcare system.
In conclusion, this study quantifies the scale of healthcare service utilization and medication use among patients with AD. Consistently higher healthcare service and medication use were observed among patients with AD compared with the general population of patients at CHS. This study therefore contributes important pre-biologic epidemiological data regarding AD in Israel.
This study was funded by an independent research grant from Sanofi. The company was not involved in the study design, execution, or manuscript preparation.
Conflicts of interest: AC served as an advisor, investigator, or speaker for Abbvie, BI, Dexcel Pharma, Janssen, Novartis, Perrigo, Pfizer, and Rafa. None of the other authors have any conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize